


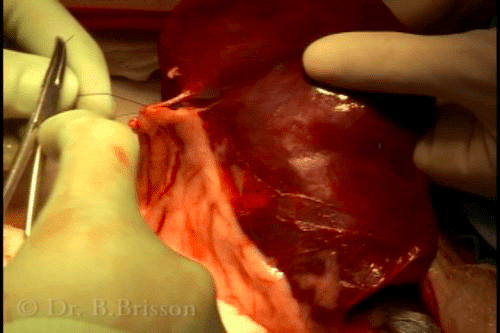
Total splenectomy is most common and is performed by ligating, stapling or sealing (using a vessel sealing device) all the hilar vessels close to the body of the spleen. Begin at the head or tail of the spleen; typically the tip that is most easily exteriorized and mobilized. Identify and dissect each hilar vessel close to the spleen. This is most easily achieved using a curved mosquito forceps.
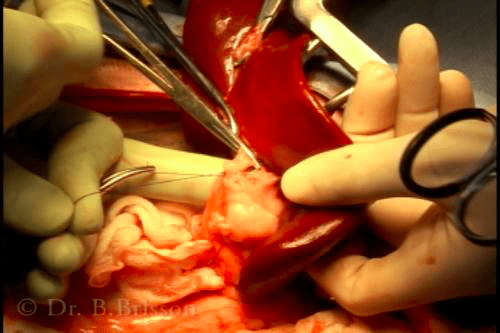
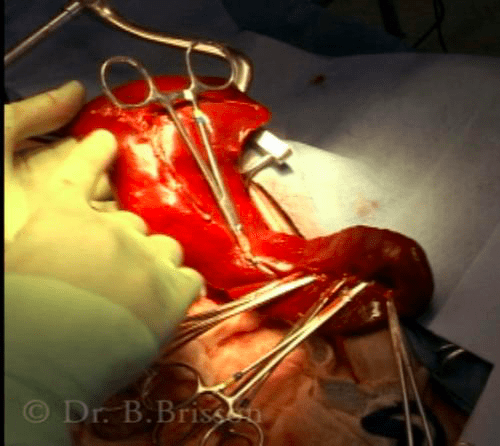
When ligatures are used, each vessel is double-ligated using 3-0 or 2-0 monfilament absorbable suture and the vessel is transected between the two ligatures leaving a small vessel stump on the abdominal side to prevent suture slippage. Large vessels can be triple-ligated leaving a double ligature on the abdominal side. Bulk ligation of multiple vessels is discouraged to prevent vessel retraction and hemorrhage. To speed up ligation, a single ligature can be applied to the abdominal side of each vessel while a mosquito forceps is applied on the splenic side. This technique is useful, but the numerous mosquito forceps can be bulky and hinder ligation. It is not uncommon for omental adhesions to form along splenic tumours. If present, begin by bulk-ligating the omentum a few centimeters away from the tumour to free up the spleen for splenectomy. If hemorrhage is severe, ligation of the large splenic artery and vein is possible but should be performed as close as possible to the spleen to prevent pancreatic or gastric wall ischemia. In this instance, it is recommended to individually ligate the splenic artery and vein to prevent the rare complication of arterio-venous fistula formation. Ligation of the splenic artery and vein within the splenic ligament (rather than along the individual hilar vessels) also requires that the short gastric vessels +/- any anastomosing epiploic vessels be ligated. Stapling devices such as the LDS and vessel sealing devices (Ligasure®) are expensive but allow a more rapid splenectomy to be performed.
After removing the spleen, inspect the splenic ligament to ensure that none of the transected vessels are bleeding. Gastropexy has been recommended if splenectomy is performed in a large, deep-chested dog, especially if a large splenic mass is removed or after splenic torsion.