

Chapter 20: Table of Contents
Bite wounds can represent a particular challenge with regards to decision-making and their clinical management. Each patient should be assessed thoroughly for concurrent life-threatening injuries prior to addressing the wound itself.

Thoracic wounds should be covered to maintain negative pressure, which is required for effective ventilation. Rapid intubation and/or chest drain placement may be necessary for distressed patients with penetrating chest wounds. Venous access should be obtained and intravenous fluid therapy initiated. Many patients require aggressive pain management and anesthesia for appropriate wound exploration and should therefore be stabilized first. Initial wound inspection will determine the extent of tissue trauma and whether contamination is severe. If antibiotics are deemed necessary, a swab of the wound for culture and sensitivity should be obtained prior to antibiotic administration. Any evidence of thoracic puncture, abdominal penetration or cervical trauma requires surgical wound exploration.
Other soft tissue wounds should be probed and most should be surgically explored. Lavage and debridement of each wound should be performed prior to deciding whether it can be closed primarily or should be treated as an open wound.
Taking a good history will help with treatment plans. Ask the owner as to where, when and how the trauma occurred. This will aid in determining management options and potential antibiotic selection. For example: road injury, farm injury (barn, manure), dog fight, bite / puncture, gunshot. Perform a general physical examination to assess the patient’s general health, to identify other concurrent injuries and to further evaluate the wound.
Recognize the type of wound:
- Laceration: sharp edges, linear or jagged edges. Minimal tissue necrosis or compression.
- Avulsion: tissue that has been pulled free of its natural attachments. Results from tensile forces and tissue damage may be mild to severe.
- Shearing: results from obliquely directed forces, usually due to high friction such as a road traffic injury. Often causes severe tissue injury of variable depth that can include underlying bone and soft tissues.
- Puncture / bite: most commonly small wounds caused by teeth. Characterized by extensive compressive forces and trauma to underlying tissue, and often involve disruption of tissue planes and large amounts of dead space even if not evident on the surface. Bacteria and even pieces of skin and hair are often deposited deep in the wound. Dog bites typically create small superficial wounds with extensive crushing and shearing damage to the underlying tissues that may or may not be appreciable initially (‘tip of the iceberg’).
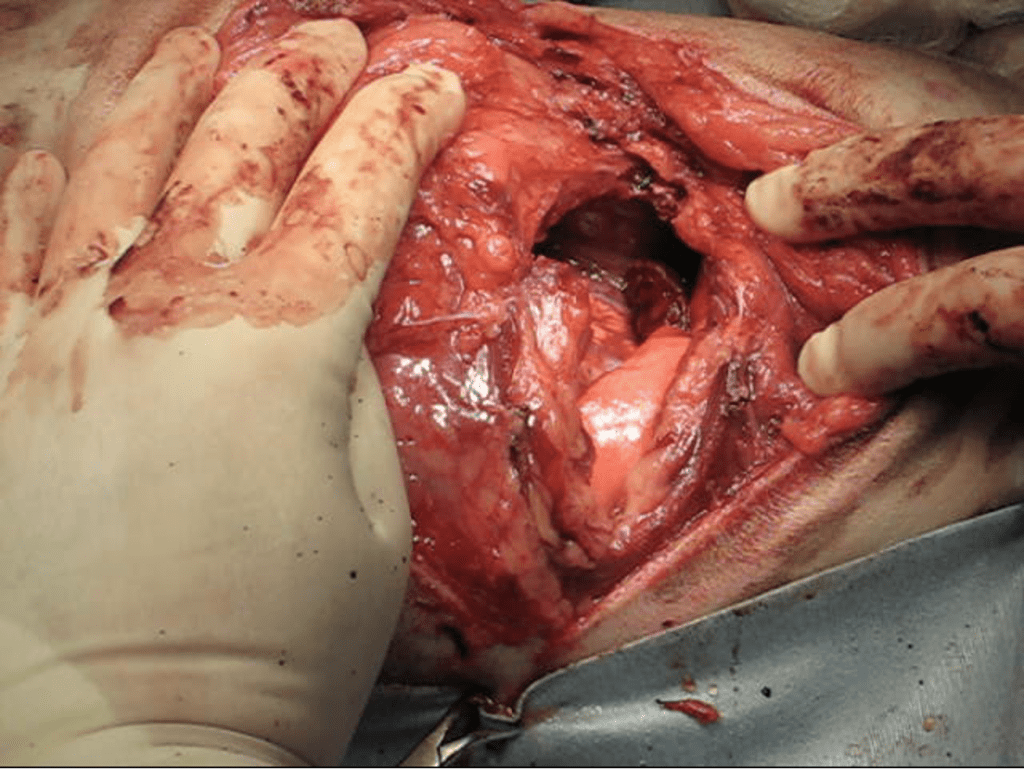
*The severity of injury is frequently underestimated; extensive damage to underlying tissues can occur even without actual skin penetration. Fractures of limbs, ribs or skull are not uncommon. Wounds to the thorax may result in pneumothorax, hemothorax, lung laceration, lung contusions, or flail chest and lack of radiographic evidence of penetration (e.g. pneumothorax) does not rule-out direct penetration. Wounds to the abdomen may result in organ trauma such as mesenteric avulsion and body wall defects that can lead to organ herniation. Failure to explore, debride and lavage wounds that contain severe necrotic tissue, with or without contamination, can lead to severe systemic disease, sepsis, disseminated intravascular coagulation (DIC) and death. As such, it is essential to fully explore the extent of tissue injury, to determine if the wound communicates with a body cavity, the extent of associated muscle or bone injury, and the presence of tissue “pockets” or dead space. Bite wounds over the body and neck should be debrided (remove necrotic tissue), cultured, lavaged and often drains inserted prior to closure.
* Any bite wound over the thoracic region should be surgically explored with the anticipation of possible thoracic penetration, severe muscle trauma +/- rib fractures, pneumo/hemothorax and the need for mechanical ventilation. Any bite wound over the abdominal cavity should also be explored since severe organ trauma can be present despite minimal externally visible tissue damage.
- Penetrating /puncture wound: injury that occurs when an object punctures the skin creating an open wound. Occurs secondary to sticks, knives, bullets and others. Bacteria can be deposited deep into penetrating wounds. Foreign material is also frequently retained (e.g. stick injuries) and may be difficult to identify, especially later down the line.
- Pressure necrosis: common complication of bandage applied too tightly (typically on limbs), and of immobilized, recumbent animals (typically on bony prominences; pressure sores).
Clinical signs include: hemorrhage, especially if footpads or large vessels are lacerated. Exposed tendons, bone or joint surfaces. Fractures and significant lameness from associated trauma. Dyspnea from thoracic wounds, especially penetrating wounds if pneumothorax, hemothorax, fractured ribs are present. Subcutaneous emphysema, from penetrating wounds, pneumothorax or severe avulsion of underlying tissue planes.
Depending on degree of injury, a balanced analgesic protocol should be initiated as soon as possible. If non-ambulatory, assessing neurologic function prior to sedation is advised (if feasible). Many patients will require surgical intervention and effective pre-operative pain management will prevent ‘wind-up’ reducing intra-operative and post-operative analgesic requirements, shorten hospital stay and generally results in better outcomes. Non-steroidal anti-inflammatories should be avoided until all concerns for ongoing hemorrhage, hypotension, and trauma to the urinary or gastrointestinal tract have been ruled-out and there are no contra-indications based on history or biochemical profile. Where there are no contraindications NSAIDs are excellent analgesics for these patients.