


Chapter 20: Table of Contents
Initial Wound Management
After patient stabilization, anesthesia is frequently required for initial wound exploration and decontamination.
What you will need:
- Sterile water-soluble lubricant (i.e. KY jelly) – use a new tube!
- Clippers
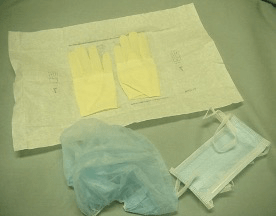
- Sterile gloves (and surgery cap and mask) to decrease the risk of iatrogenic contamination with resistant hospital bacteria which are present in all clinics
- Sterile surgical instruments for debridement: tissue forceps, Metzenbaum and/or Mayo scissors, hemostatic clamps, scalpel blade, +/- needle drivers and suture (monofilament) / skin staples
- 35 mL syringe with an 18 gauge needle or intravenous catheter
- Lavage solution (LRS is ideal but sterile saline will do)
Apply sterile water-soluble lubricant to the wound surface +/- cover with gauze to help protect it from hair contamination during clipping. For large wounds, sterile gauze can be packed into wound site for protection. Clip hair from around the wound site and surrounding body regions – clip liberally (at least 5-10 cm beyond wound margin or the entire circumference if on an extremity).



Initial gross cleaning: The skin surface surrounding the wound should be cleaned with an antiseptic scrub (i.e. chlorhexidine soap brush). Direct contact with the wound should be avoided. A standard skin preparation using alcohol and/or chlorhexidine can be performed on the skin surrounding the wound (area that will be included in the surgical field or bandage) but there should be no contact with the wound.
Prior to proceeding with lavage of the wound, sterile hemostats or other fine instrument and tissue forceps are used to carefully probe the extent of the wound to determine the following:
- Whether it communicates with a body cavity (i.e. chest, abdomen) – realizing that a communication may not be identified even if it exists.
- Depth and extent of wound involvement (assessing possible dead space).
- Damage to underlying tissue planes and muscles.
- Presence of debris or necrotic tissue deep within the wound (may not be appreciated without complete exploration) and flushing could push this tissue deeper into the wound.
*Wound exploration is especially important to perform for penetrating or puncture/bite wounds where tissue damage may be more severe than anticipated.