

Chapter 20: Table of Contents
Wounds to the neck / thorax may cause pneumothorax, hemothorax, lung laceration, lung contusions, rib fractures or flail chest. Thoracic wounds often require extensive debridement of devitalized tissue (e.g. subcutaneous tissue and intercostal muscles) and reconstruction in order to re-align fractured rib segmnents and re-establish negative pressure in the thoracic cavity. Small wounds over the thoracic cavity do not necessitate emergency exploratory thoracotomy unless the patient cannot be stabilized but all thoracic wounds should be surgically explored in a timely fashion with the anticipation of possible thoracic penetration and the need for mechanical ventilation. Thoracic wounds often require extensive debridement of devitalized tissue and reconstruction in order to reestablish a closed cavity, if you do not feel comfortable exploring and managing such extensive wounds (that may require a thoracotomy), these patients should be referred as soon as possible after initial stabilization.
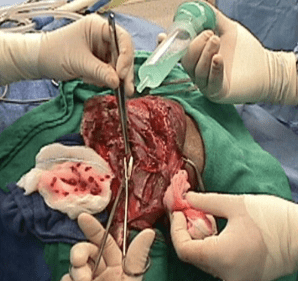
Prior to closure, the thoracic cavity, as well as the wound bed, are lavaged repeatedly with warm sterile 0.9% saline solution. Most cases will require a chest tube to provide postoperative drainage of inflammatory fluid and help reestablish negative pressure. Due to extensive soft tissue trauma, further drainage of the subcutaneous and muscle layers is also often necessary. Closed suction drains (Jackson-Pratt) should be used instead of Penrose drains to prevent potential entry of air or environmental contaminants into the chest cavity. Drainage is especially important with bite wounds due to the inherent tissue contamination and the frequently extensive tissue trauma.