


Chapter 20: Table of Contents
Abdominal Cavity Penetration
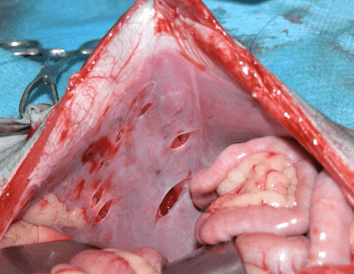
A laparotomy is indicated for wounds that penetrate the abdomen. Crushing and tensile forces may cause abdominal wall rupture leading to herniation. Compromise to the small or large intestine with devitalization of these tissues over 12-72 hours after trauma is also possible. Areas of discoloured intestines should be resected along with any necrotic or devitalized fat or omentum. Tears or perforations of multiple abdominal organs are frequent, splenic laceration and hemorrhage, pancreatic damage, renal contusions, and bladder rupture are not uncommon. Full-thickness abdominal wall wounds may be debrided and the body wall closed from the laparotomy approach, and the superficial (overlying) tissues managed by external debridement, lavage and closure or bandaging and open wound care. Before closing, the abdomen should be copiously lavaged with warm 0.9% sterile saline solution. If abdominal penetration was confirmed placement of an active suction drain (Jackson Pratt drain) is recommended. The drain can be removed soon after surgery if fluid production is minimal, but ideally only once the results of culture and sensitivity are available. Collection of abdominal drainage fluid postoperatively allows for diagnostic cytology and bacterial culture when monitoring for evidence of post-operative peritonitis. Referral to a specialist is recommended after stabilization if the clinician is not prepared or comfortable with managing advanced abdominal procedures and postoperative management of a critical patient.