


Chapter 22: Table of Contents
Subcutaneous Ureteral Bypass (SUB)
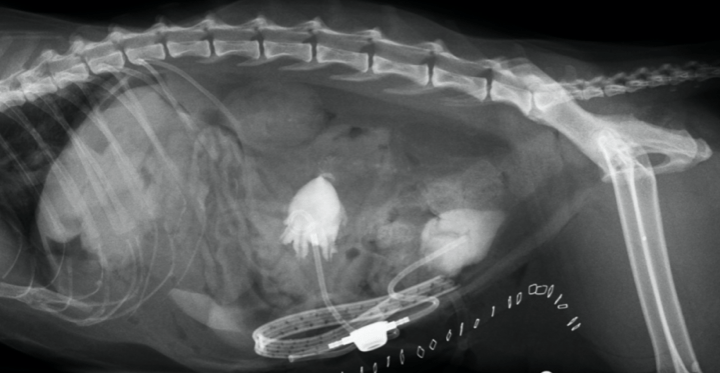
The SUB device was developed to allow bypassing the compromised ureter completely. It consists of a nephrostomy catheter and a cystostomy catheter joined subcutaneously by an injection port. This latter allows for sterile urine collection (for culture and / or urinalysis), flushing and contrast studies to be performed. The SUB system is available in two sizes, a smaller system for small dogs and cats and a larger system for larger dogs. (Norfolk Vet Products)
SUBs have become the go to option for cats with unilateral or bilateral ureteral obstruction, ureteral stenosis in which case a stent cannot be passed, or when stenting was not tolerated or a stent has migrated. In dogs, ureteral stenting is the preferred first option followed by SUB if stenting has failed or is not feasible.
Contraindications to SUB placement include severe coagulopathies and severe hydronephrosis, though marked hydronephrosis is still compatible with SUB placement. Though some references indicate that a minimum renal pelvis dilation of 5mm is required for implantation, the SUB can be implanted in a kidney with lesser to no dilation.
SUB placement is performed using a laparotomy approach. It is ideal to implant the device in urine that is void of infection but this is not always possible. Urine culture is typically submitted preoperatively but results are not always available due to the emergent need for surgery. Intraoperatively, urine is collected from the renal pelvis and a contrast pyelo-ureterogram is performed (using fluoroscopy) to confirm the obstruction and it’s location. Following this, the nephrostomy catheter is inserted under fluoroscopic guidance into the kidney and either curled into the dilated renal pelvis or advanced into the proximal ureter. The nephrostomy tube Dacron cuff is glued to the renal capsule. The cytstostomy is inserted next (sutured and glued to the bladder), followed by the joining subcutaneous port. The port is sutured in place and tested for patency and leakage under fluoroscopic guidance prior to abdominal closure. Extreme aseptic technique is required to prevent infection of this system and gentle manipulation of the kidney is required to prevent further renal damage.
Postoperatively, bloodwork is monitored with the expectation of seeing a rapid decrease in renal values related to the relief of the obstruction. Patients typically remain in hospital on fluid therapy until electrolytes and renal values have improved, and patients can be managed on oral pain and other medications at home. Renal values that remain stagnant or do not drop back into normal ranges may be due to complications or to permanent loss of renal function.
Postoperatively, fluid therapy is continued as well as antibiotic therapy (typically marbofloxacin) for a period of 2-4 weeks based on culture and sensitivity results.
Potential complications associated with SUB placement include: Inappropriate placement, urine leakage, renal hemorrhage during placement or postoperatively which can lead to obstruction by a blood clot, dislodgement of either ostomy catheter, kinking of the system, dysuria, discomfort and intermittent hematuria related to the presence of the cystostomy catheter, obstruction due to stones, urinary tract or SUB system infection (which can be chronic).
Long-term SUB care includes reevaluations at 1 month and every 3 months for the first year, followed by rechecks every 3-6 months thereafter. At each visit, a urine culture +/- cytology is performed and the SUB is flushed to confirm patency and to reduce the risk of future obstruction. SUB flushes are typically performed using aseptic technique and are performed under ultrasound guidance, by a user, trained in SUB maintenance.
Surgical outcomes after SUB placement are quite good with as many as 100% of cases (Horowitz et al. 2013) having successful decompression and continued system patency at average follow-up of 19 months (Deroy 2017) and most showing improved renal parameters postoperatively.
< Ureteral Stenting Stent vs. SUB >
References:
Deroy C, Rossetti D, Ragetly G, et al. Comparison between double-pigtail ureteral stents and ureteral bypass devices for treatment of ureterolithiasis in cats. JAVMA 2017; 251:429-437.
Horowitz C, Berent A, Weisse C, et al. Predictors of outcome for cats with ureteral obstructions after interventional management using ureteral stents or a subcutaneous ureteral bypass device. J Feline Med Surg 2013; 15:1052-1062.