


Chapter 2: Table of Contents
Skin Preparation
The goal of patient skin preparation is to reduce the transient bacterial flora on the skin surrounding the surgical incision site to decrease the risk of incisional infection.
Typical skin preparation includes a 5 minute soap scrub followed by the application of alcohol and finally an alcohol based disinfectant such as chlorhexidine.
When disinfecting a wound or a surgical site that is close to, or includes mucous membranes, alcohol is not used and the disinfectant used is typically water (aqueous) based instead.
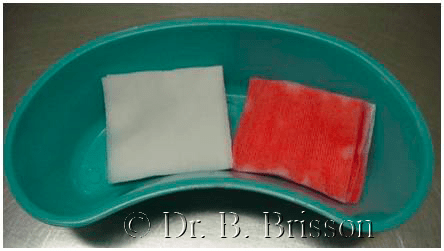
In a kidney dish, place two chlorhexidine soaked scrub brushes in warm tap water. In another, place two piles of gauze sponges and thoroughly soak each one with isopropyl alcohol and with a chlorhexidine based tincture respectively in preparation for patient preparation.
Step 1: Soap Scrub
The skin is prepared to mechanically remove oil and debris and to reduce the transient bacterial flora on the skin surrounding the proposed surgical incision site. A disinfectant soap is used in the first step of skin preparation. Commonly used soaps for preparing surgical patients contain chlorhexidine or povidone-iodophors as the main antibacterial agent.
After removing or replacing the labcoat worn during clipping and vacuuming, an initial soap scrub is performed. At the OVC, two consecutive soap scrubs (using two separate scrub brushes soaked with tap water), are performed while doning non sterile exam gloves (total of 5 minutes contact time). Use only the sponge side of the brush.
A first brush is used to create a lather and remove superficial dirt and debris. Prior to discarding it, the first brush is also often used to wet and comb (this time using the bristle side of the brush) the hair adjacent to the field so it is oriented away from the surgical site. This first soap scrub is removed using paper towels or gauze. While still doning exam gloves, a second water and chlorhexidine soaked scrub brush is used to perform the second soap scrub. It is important to create a good lather (suds) over the entire field to allow good contact between the antiseptic soap and the skin. As long as the soap is in contact with the skin, you do not need to physically scrub the skin for the entire time period if the skin is clear of debris as this may abrade the skin excessively. A hat and mask is often worn during this portion of the prep. In private practice, gauze sponges soaked with disinfectant soap and tap water (instead of scrub brushes) are commonly used to perform the soap scrub.
STEP 2: Wipe Suds
After the soap scrub is complete (5 minutes of suds contact time), the suds are removed using a clean paper towel or a gauze sponge in order to perform the next steps of skin preparation.
Then, depending on the solution used to perform the soap scrub, perform the circumferential preparation using alcohol and tincture of chlorhexidine swabs (or alcohol and tincture of iodine swabs if that is what your practice uses).
Skin preparation generally begins at the center of the shaved area (at the proposed incision site), and continues using a concentric circular pattern until the edges of the shaved area are contacted. Remember never to return towards the incision site with used gauze; once hair is touched, the gauze or cotton is discarded and a new one is used. This action is repeated over the entire field a minimum of three timesfor each solution. Cover the surgical field with a sterile drape or towel to prevent contamination of the prepared surgical field during transfer to the surgical suite.
Two types of preparation patterns:
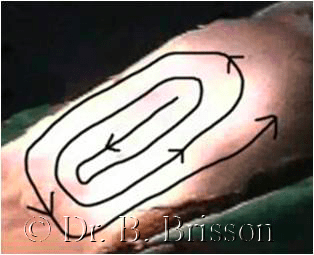
1) Concentric Preparation: Skin preparation generally begins at the center of the shaved area, (at the proposed incision site), and continues using a concentric circular pattern until the edges of the shaved area are contacted. Remember never to return towards the incision site with a used gauze. Once hair is touched, the gauze or cotton is discarded and a new gauze is used. This action is repeated over the entire field a minimum of three times.
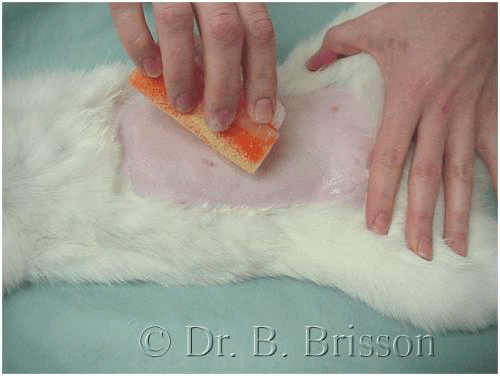
2) Horizontal Preparation: Skin preparation generally begins at the center of the shaved area, (at the proposed incision site), and continues using a horizontal pattern on either side of the shaved area. One must remember to never return towards the incision site with a used gauze. If hair is touched (at the top or the sides of the incision), the gauze or cotton is discarded and a new gauze is used. This action is repeated over the entire field a minimum of three times.
Step 3: Alcohol

The second step of skin preparation involves removing the lather formed during scrubbing by wiping with isopropyl alcohol soaked gauze swabs or cotton balls. Alcohol disinfects and helps to dissolve oils from the skin.
Step 4: Disinfectant

Disinfectants are then applied to the surgical site to allow further bacterial killing to occur. These products usually contain the same active agents as the soaps used for the surgical scrub (e.g. chlorhexidine), but are more concentrated and usually contain alcohol as a base. The disinfectant is painted on the skin with a cotton ball, gauze swab or may be sprayed on. Some disinfectants such as iodophors require a longer contact time (2 minutes) to be effective. Aqueous (non alcohol based) solutions are used to prepare wounds or surgical sites that are close to, or include mucous membranes.
Sterile Draping:
Prior to transporting the patient to the surgical suite, the prepared surgical site is covered using a sterile drape or towel to prevent inadvertent contamination during transportation.
Remember: Surgically prepared skin is very clean but is never sterile.
Final Skin Preparation (Performed After Scrubbing, Gowning and Gloving)
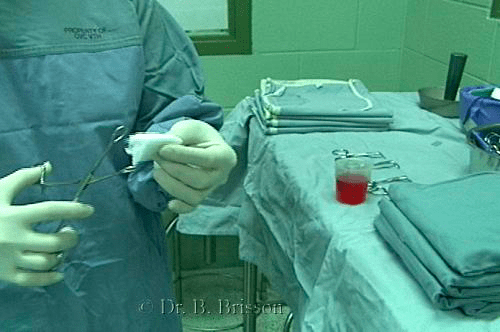
Following initial skin preparation and transport to the surgical suite, the gowned (and gloved) surgeon performs final skin preparation prior to applying the surgical drapes. A sterile gauze sponge is grasped using sterile sponge forceps. The sponge is then dipped in an antiseptic solution (iodine or chlorhexidine based tincture depending on the solution used for skin preparation) and the site is prepared using a concentric pattern as previously described. The surgeon should be careful not to contaminate the sterile surgical gown (or gloves) on the surgical table, patient (especially hair) or anesthesia equipment during final preparation. Once final preparation is complete, the gauze and sponge forceps are discarded without handling or passing over the surgical table (come from behind) since they are no longer considered sterile.