


Chapter 14: Table of Contents
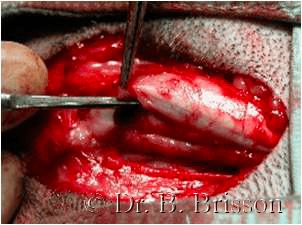
Prescrotal urethrotomy is most commonly performed due to the location of the obstruction just caudal to the os penis although in some instances, penile or perineal urethrotomy is necessary. Urethrotomy is most commonly performed under general anesthesia but can be performed under sedation and local anesthesia in unstable patients. With the patient in dorsal recumbency, the prescrotal area is clipped and prepared for surgery. I typically advance a 5 or 8 French, flexible, sterile urinary catheter to the level of the obstruction. Make a midline incision over the affected urethra; you should be able to palpate the stones just caudal to the os penis. Cut through the skin and subcutaneous tissues. The retractor penile muscle covers the urethra at the level of the pre-scrotal and scrotal urethra; this muscle must be retracted laterally to identify the urethral wall. The urethra can be visualized as a blueish tubular structure of variable diameter. Palpation of the calculi or catheter can help identify the urethra. Make a 1-2 cm midline urethral incision overtop and just cranial (in the distended urethra) to the obstruction; be sure not to cut the dorsal wall of the urethra. The urethral wall is quite vascular – hemorrhage is normal. Apply pressure with a gauze sponge to absorb any blood and slow the hemorrhage but do not coagulate or ligate the urethral edges. Remove the urethral calculi with a small hemostatic forceps or a curette, flush with warm saline and gently advance the urinary catheter into the bladder. Retropulsion may be necessary to dislodge smaller calculi or those located more proximally along the urethra; a cystotomy will be necessary to remove these calculi. I leave the urinary catheter in place until the cystotomy is performed (if necessary) to prevent cystic calculi from migrating back into the urethra. Urethrotomy incisions are not typically sutured but rather left to heal by second intention (without postoperative catheterization). This type of healing rarely leads to stricture or infection. However, intermittent hemorrhage, mostly associated with urination or excitement, should be expected for 3-5 days postoperatively. Patients with coagulopathies such as Dobermans with von Willebrand’s disease should undergo closure of the urethrotomy site. Closure is performed over a urinary catheter using 4-0 or 5-0 absorbable suture material in a simple interrupted pattern. Closure of the subcutaneous tissues and skin are routine. Regardless of whether you close the urethrotomy site or let it heal by second intention, all patients should wear an E-collar for 7-10 days or until the site has healed. A study comparing sutured and non-sutured urethral incisions revealed more fibrosis and less inflammation at 3 and 6 weeks postoperatively in the group that healed by second intention compared to the sutured group. (Weber 1985) Stricture did not occur in any dog. (Weber 1985)