


Chapter 11: Table of Contents
- 11.1 Intestinal Biopsy
- 11.2 Intestinal Biopsy Quiz
- 11.3 Intestinal Resection and Anastomosis
- Intestinal Apposition and Closure
- Suture the mesenteric rent, leak test, and omentalize
- Video: Intestinal Resection and Anastomosis
- How to accommodate discrepancies in luminal size when performing a resection-anastomosis
- Decision-making in the management of gastrointestinal foreign bodies
- Decision-making in the management of gastrointestinal foreign bodies: continued
- Decision-making in the management of gastrointestinal foreign bodies continued
- Enterotomy vs. Resection-Anastomosis
- Assessing Intestinal Viability
- Where to incise when removing a focal foreign body via enterotomy?
- Linear foreign body removal
- Where to cut when performing a resection-anastomosis
- Prognosis- foreign body
- Complications
- Use of Antibiotics?
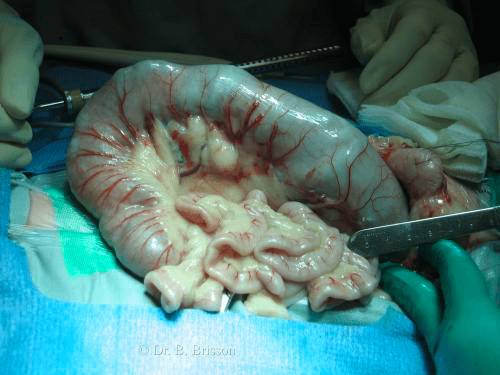
Assessing Intestinal Viability
Several tests such as fluoresceine dye injection and surface oximetry have been used to help determine gastric and intestinal viability in animals and in people. In daily practice, the decision is made using the following subjective criteria:
- Colour: Viable intestinal loops are often red, red-blue, even purple. If the intestinal wall is gray, green, dark purple or black, it should be resected. In addition, the colour should improve after the foreign body is removed and the luminal pressure is released (e.g. from red-blue to red). Irrigation with warm saline may also improve the colour of viable intestine.
- Wall thickness: Intestinal wall palpation should reveal a normal or increased (swelling) wall thickness compared to the remainder of the adjacent intestine. Palpation of a thin intestinal wall is an indication for resection.
- Peristalsis: Viable intestinal wall is able to initiate and propagate a peristaltic wave. If peristalsis is not noted, gently pinch the intestine in the affected area, this should initiate a peristaltic wave. Note that peristalsis may be affected by long-standing obstruction, ileus and anesthetic drugs.
- Arterial pulses: Arterial and venous thrombosis is a strong indication for resection; look for strong arterial pulses in the vessels supplying the affected area. Lack of arterial bleeding at the cut edge is an indication for resection.
< Enterotomy vs Resection-Anastomosis Where to incise when removing a focal foreign body via enterotomy >