Chapter 11: Table of Contents
- 11.1 Intestinal Biopsy
- 11.2 Intestinal Biopsy Quiz
- 11.3 Intestinal Resection and Anastomosis
- Intestinal Apposition and Closure
- Suture the mesenteric rent, leak test, and omentalize
- Video: Intestinal Resection and Anastomosis
- How to accommodate discrepancies in luminal size when performing a resection-anastomosis
- Decision-making in the management of gastrointestinal foreign bodies
- Decision-making in the management of gastrointestinal foreign bodies: continued
- Decision-making in the management of gastrointestinal foreign bodies continued
- Enterotomy vs. Resection-Anastomosis
- Assessing Intestinal Viability
- Where to incise when removing a focal foreign body via enterotomy?
- Linear foreign body removal
- Where to cut when performing a resection-anastomosis
- Prognosis- foreign body
- Complications
- Use of Antibiotics?
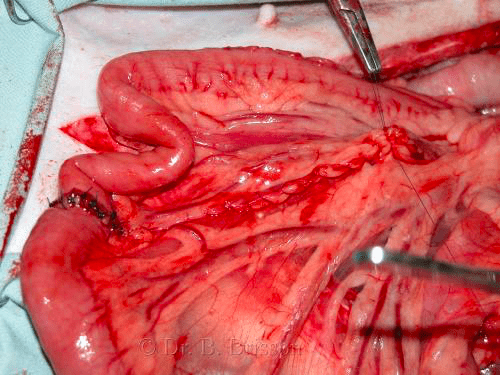
Where to cut when performing a resection-anastomosis
Transect the intestine in a ‘viable’ area. Cut the bowel ends at an angle (longer on the mesenteric border than on the antimesenteric border) to ensure good blood supply to the intestinal anastomosis. If the tissues at the cut end don’t look healthy, remove more. All of the grossly abnormal intestine should ideally be removed. This becomes difficult in cases with extensive intestinal trauma caused by linear foreign bodies since resection of 70-80% of the small intestinal length or more results in short-bowel syndrome. Because short bowel syndrome leads to severe diarrhea, bacterial overgrowth and weight loss, the surgeon must, in some cases, cut the intestine in a less than ideal location to allow for enough intestinal length to remain; this obviously increases the risk of dehiscence.