


Chapter 11: Table of Contents
- 11.1 Intestinal Biopsy
- 11.2 Intestinal Biopsy Quiz
- 11.3 Intestinal Resection and Anastomosis
- Intestinal Apposition and Closure
- Suture the mesenteric rent, leak test, and omentalize
- Video: Intestinal Resection and Anastomosis
- How to accommodate discrepancies in luminal size when performing a resection-anastomosis
- Decision-making in the management of gastrointestinal foreign bodies
- Decision-making in the management of gastrointestinal foreign bodies: continued
- Decision-making in the management of gastrointestinal foreign bodies continued
- Enterotomy vs. Resection-Anastomosis
- Assessing Intestinal Viability
- Where to incise when removing a focal foreign body via enterotomy?
- Linear foreign body removal
- Where to cut when performing a resection-anastomosis
- Prognosis- foreign body
- Complications
- Use of Antibiotics?
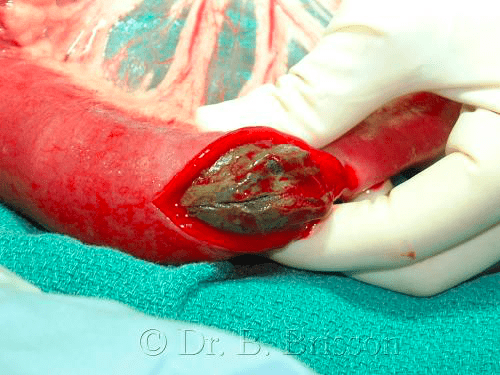
Enterotomy vs. Resection-Anastomosis
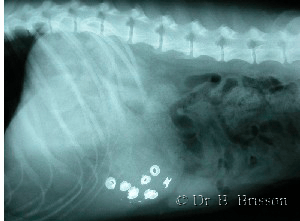
Gastric foreign bodies are removed by gastrotomy (see the section on gastrotomy). I have yet to resect a portion of the stomach secondary to a foreign body. In contrast, intestinal foreign bodies can cause significant devitalization of the affected loops of bowel, which may need to be resected. Therefore, the questions to ask when evaluating a patient with an intestinal foreign body are: 1) whether or not the affected intestine is viable (enterotomy vs resection-anastomosis) and 2) if the intestine is not viable, how much intestine must be resected. Unless the tissues are obviously necrotic, viability is often difficult to determine. If I have any doubt as to whether or not the intestinal loop is viable, I resect it. In some instances, I perform an enterotomy to remove the foreign body and I reassess viability after the intraluminal pressure has been reduced. If I am unsure about viability using the criteria described below, I proceed with a resection-anastomosis.
If the intestine is viable, I perform an enterotomy since the rate of dehiscence with resection-anastomosis is reportedly higher than that associated with an enterotomy (Allen 1992). The rate of dehiscence is also higher in patients that receive an enterotomy for foreign body removal compared to biopsy (Allen 1992, Weisman 1999) and when more than one enterotomy or resection-anastomosis is performed (Wylie 1994).
< Decision-making in the management of gastrointestinal foreign bodies continued Assessing Intestinal Viability >