


Chapter 11: Table of Contents
- 11.1 Intestinal Biopsy
- 11.2 Intestinal Biopsy Quiz
- 11.3 Intestinal Resection and Anastomosis
- Intestinal Apposition and Closure
- Suture the mesenteric rent, leak test, and omentalize
- Video: Intestinal Resection and Anastomosis
- How to accommodate discrepancies in luminal size when performing a resection-anastomosis
- Decision-making in the management of gastrointestinal foreign bodies
- Decision-making in the management of gastrointestinal foreign bodies: continued
- Decision-making in the management of gastrointestinal foreign bodies continued
- Enterotomy vs. Resection-Anastomosis
- Assessing Intestinal Viability
- Where to incise when removing a focal foreign body via enterotomy?
- Linear foreign body removal
- Where to cut when performing a resection-anastomosis
- Prognosis- foreign body
- Complications
- Use of Antibiotics?
Intestinal Apposition and Closure
- Use monofilament, absorbable suture such as Biosyn®, PDS®, or Maxon® on a taper or taper-cut needle and apply 4-5 throws to each knot. Do not use chromic gut for gastrointestinal surgery. Non absorbable, monofilament suture can be used in hypoalbuminemic patients or patients anticipated to have delayed wound healing but this is unnecessary.
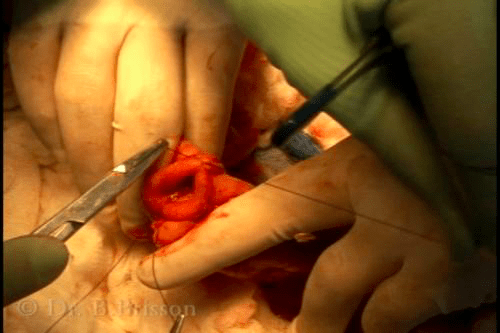
- Do not pick up the intestinal wall with thumb forceps. Instead, insert the tip of your forceps within the lumen to create counter pressure while puncturing the wall with the suture needle. Any trauma at the anastomosis site will increase the risk of postoperative dehiscence.
- Include the entire intestinal wall in your suture bites. Alternatively, include all layers but the mucosa. The submucosa is the layer of strength and must be included in all bites. I take full thickness bites and I angle my suture bite to include more serosa than mucosa – this helps reduce mucosal eversion. The mucosa can also be trimmed with Metzembaum scissors as required. Alternatively, engage the entire wall thickness, then retract the needle slightly to let the mucosa slip out and begin the bite on the opposite side just between the muscosa and submucosa to help invert the mucosal layer.
- Appositional, simple interrupted pattern with 3-4 mm wide bites and sutures placed 2-3 mm apart is the typical closure pattern. All knots are extra-luminal.
- I apply a surgeon’s throw to prevent loosening while I place my second suture throw if the knot wants to loosen under tension. This is typically only necessary for the 12, 3, 6 and 9 o’clock sutures. Tighten the suture enough to appose the tissues but do not crush or strangulate.
< Intestinal Resection and Anastomosis Intestinal Apposition and Closure, Continued >