


Chapter 11: Table of Contents
- 11.1 Intestinal Biopsy
- 11.2 Intestinal Biopsy Quiz
- 11.3 Intestinal Resection and Anastomosis
- Intestinal Apposition and Closure
- Suture the mesenteric rent, leak test, and omentalize
- Video: Intestinal Resection and Anastomosis
- How to accommodate discrepancies in luminal size when performing a resection-anastomosis
- Decision-making in the management of gastrointestinal foreign bodies
- Decision-making in the management of gastrointestinal foreign bodies: continued
- Decision-making in the management of gastrointestinal foreign bodies continued
- Enterotomy vs. Resection-Anastomosis
- Assessing Intestinal Viability
- Where to incise when removing a focal foreign body via enterotomy?
- Linear foreign body removal
- Where to cut when performing a resection-anastomosis
- Prognosis- foreign body
- Complications
- Use of Antibiotics?
Intestinal Apposition and Closure- Continued
- Other techniques include simple continuous appositional suture pattern and stapled anastomoses. Continuous closure is as safe as interrupted if performed correctly. Begin by tying a strand of suture at the mesenteric junction and one at the antimesenteric junction – use the suture ends to stretch-out the lumen. Perform two continuous suture lines; one from the mesenteric border to the antimesenteric border on the first side and a second in the opposite direction on the opposite side. Performing two separate continuous lines instead of one reduces the risk of purse string effect on the luminal diameter. Use absorbable suture material for continuous closure since non-absorbable suture has been associated with entrapment of foreign bodies. Skin staples have been used experimentally to perform end-to-end anastomoses (Coolman 2000); I have no experience with this technique, but it reportedly produces strong anastomoses. Other specialized stapled equipment can be used to perform anastomoses but are very expensive.
- When performing an end-to-end anastomosis, I place my first suture at the mesenteric border (6 o’clock position) followed by a suture immediately adjacent to this one on either side (~5 o’clock and 7 o’clock position); this is where leaks occur most commonly. Then I place a suture at the antimesenteric border (12 o’clock position), followed by sutures at the 3 o’clock and 9 o’clock positions to divide the luminal diameter evenly. Once this is done, I fill in the gaps until the entire circumference is sutured.
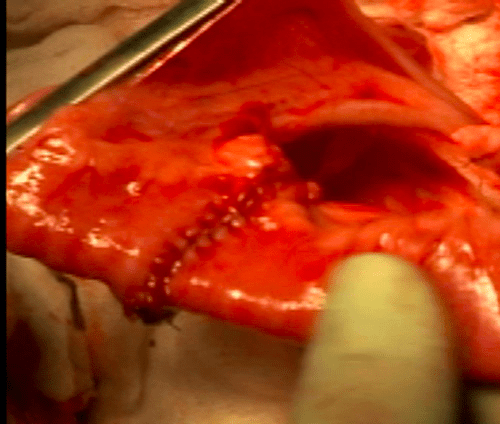
<Intestinal Apposition and Closure Suture the Mesenteric Rent, Leak Test and Omentalize >