

Chapter 11: Table of Contents
- 11.1 Intestinal Biopsy
- 11.2 Intestinal Biopsy Quiz
- 11.3 Intestinal Resection and Anastomosis
- Intestinal Apposition and Closure
- Suture the mesenteric rent, leak test, and omentalize
- Video: Intestinal Resection and Anastomosis
- How to accommodate discrepancies in luminal size when performing a resection-anastomosis
- Decision-making in the management of gastrointestinal foreign bodies
- Decision-making in the management of gastrointestinal foreign bodies: continued
- Decision-making in the management of gastrointestinal foreign bodies continued
- Enterotomy vs. Resection-Anastomosis
- Assessing Intestinal Viability
- Where to incise when removing a focal foreign body via enterotomy?
- Linear foreign body removal
- Where to cut when performing a resection-anastomosis
- Prognosis- foreign body
- Complications
- Use of Antibiotics?
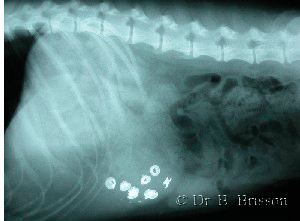
Decision-making in the management of gastrointestinal foreign bodies
Conservative management of relatively small radioopaque foreign bodies is possible but surgery is indicated if: vomiting persists; the patient’s clinical status deteriorates; the foreign body does not move for 6-8 hours; or, the foreign body has not reached the colon within 36 hours. Gastric foreign bodies are not usually considered a surgical emergency but intestinal foreign bodies generally are.
Patients suspected of having a gastrointestinal foreign body should be explored through a large laparotomy incision which allows easy exploration of all aspects of the gastrointestinal tract and manipulation of organs without trauma. As indicated for most abdominal procedures, the falciform ligament should be removed to improve surgical visualization. The entire gastrointestinal tract should be examined and palpated since more than one foreign body may be present. Unless rupture is identified, the entire tract should be assessed prior to performing any intervention along the gastrointestinal tract (to reduce contamination).
< How to Accommodate Discrepancies in Luminal Size When Performing a Resection- Anastomosis Decision Making in the Management of Gastrointestinal Foreign Bodies, Continued >