

Chapter 11: Table of Contents
- 11.1 Intestinal Biopsy
- 11.2 Intestinal Biopsy Quiz
- 11.3 Intestinal Resection and Anastomosis
- Intestinal Apposition and Closure
- Suture the mesenteric rent, leak test, and omentalize
- Video: Intestinal Resection and Anastomosis
- How to accommodate discrepancies in luminal size when performing a resection-anastomosis
- Decision-making in the management of gastrointestinal foreign bodies
- Decision-making in the management of gastrointestinal foreign bodies: continued
- Decision-making in the management of gastrointestinal foreign bodies continued
- Enterotomy vs. Resection-Anastomosis
- Assessing Intestinal Viability
- Where to incise when removing a focal foreign body via enterotomy?
- Linear foreign body removal
- Where to cut when performing a resection-anastomosis
- Prognosis- foreign body
- Complications
- Use of Antibiotics?
Decision-making in the management of gastrointestinal foreign bodies: continued
Some foreign bodies will remain in the stomach; others will migrate through the small intestines. Most obstructions caused by focal foreign bodies (toys, corn cob, peach pit, etc.) occur in the jejunum. However, it is possible that the foreign body was initially lodged somewhere orad to the current site of obstruction; examine all the intestinal loops to identify evidence of intestinal discoloration or devitalization proximally. Foreign bodies that become lodged within the intestine create direct pressure on the intestinal wall. When complete obstruction is present, intestinal distension develops orad to the foreign body.
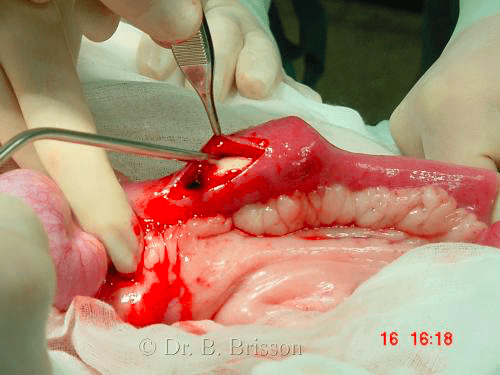
Linear foreign bodies such as ropes, nylon stocking, string and carpet are unique in that they tend to become anchored at the base of the tongue (more commonly in cats) or in the pyloric antrum (common in dogs). As peristaltic waves attempt to move the foreign body, intestinal loops surrounding the foreign body gather together in an accordion-like pattern (plication). With increasing peristalsis, the foreign body tightens and becomes embedded in the mesenteric surface of the intestine. In severe cases, the foreign body can essentially ‘saw’ through the mesenteric border of the intestinal wall leading to mesenteric ischemia, vascular damage and eventually leakage and peritonitis. Although conservative management has been described in non-clinical cats having recently ingested thread on a needle (by releasing the attachment at the base of the tongue and letting the foreign body pass on it’s own), the potential for serious complications should this fail must weighed against the cost and trauma associated with exploration and removal.

< Decision Making in the Management of Gastrointestinal Foreign Bodies Decision Making in the Management of Gastrointestinal Foreign Bodies, Continued >